How Brief Therapy Philosophy Helps Re-vision Service Pathways
“Our goal is to deliver a coordinated, responsive system that makes sense to parents and young people, that is easy to navigate, that enables fast answers and clear pathways to care. Most important of all – the system must deliver early and appropriate help for each child and youth who needs it.” -Ministry of Children and Youth Services
It has never sat right with me that children and youth should have to wait for mental health services. Yet this is the case for many communities throughout Ontario spurring the Moving on Mental Health initiative by the province. Parents have voiced their frustration with wait times for children’s mental health services as well as their confusion in regards to the pathways to services. These concerns seem well founded as the children’s mental health machine seems liken to an outdated computer operating system with lots of waiting and spinning wheels. It doesn’t have to be this way though. A review and adjustments are warranted.
Capacity Versus Demand:
As part of the conversation ‘capacity versus demand’ for service is one focal point. Certainly in many agencies the demand for service as it is currently provided does exceed the capacity to provide those services. This results in bottlenecking and families waiting for services. However are there opportunities to adjust how services are currently delivered freeing up direct service hours? This is a question proposed models such as the Choice and Partnership Approach (CAPA) has tried to address. There seems to be some important sensibilities to this model of service delivery that add to the conversation for us here in Ontario.
The Service Continuum:
An equally important focal point for this discussion is in regards to re-visioning the ‘pathways to service’ and journey through the service continuum. Currently, very often a participant begins the relationship with service through telephone interviews and assessment with the exception of the use of walk-in counselling clinics. A great deal of information is gathered that is not necessarily related to what people want different in their life. Multiple conversations are had prior to the person experiencing a face to face therapeutic encounter. If we were to approach our service as though running a business would we not want to get the product up front, utilized, and familiar to the community? In considering the service continuum the following questions may be useful:
- How can we be most responsive to the children youth and families experiencing distress?
- How do we get therapeutic services to people as soon as possible?
- How do we resist over-service where families receive not one more session than they want or need and not one less than they want or need?
- What are the service activities that take up the most amount of time yet are not relevant to what people want different in their lives?
- How can we design a pathway that is clear and simple?
- How can these pathways make visible and respond to social injustice?
- What design allies with the current research?
Value-based Planning:
Beginning this project of re-vision the first step may be to engage in value-based planning during which the personal, agency and communal values are made visible to serve as the compass for planning services. For instance all levels are invited to reflect on and archive their answers to questions such as:
- What do we want the person(s) experience at first contact to be?
- What is our preferred experience for children, youth and families through the service continuum?
- What experiences do we want to guard against?
Answers to these questions provide guidance in re-visioning services and services pathways. Serving as a compass or touch stone along the way we ensure services are consistent with what is important to the agency, employee, and community.
A Clear Philosophy:
Secondly in re-vision it is important to be clear on the guiding philosophy, that is, the ways of thinking about people, problems, change and therapy. Many agencies operate informed by a modernistic lens adopting an objective bio-medical understanding of distress positioning the service provider as expert and assessor. This welcomes processes such as the use of tools to determine streams of service, risk and priority. Often these tools administered over the phone, traffic in language consistent with a deficit focus and pathology. Families are streamed to the prescribed wait list and a great deal of time is allotted to maintaining those wait lists, triaging, further reviewing urgency and eligibility.
The Brief Therapies:
With the emergence of the walk-in counselling clinic in Ontario we have experienced a very different way of delivering counselling services. Most importantly the brief therapy philosophy opens new options for re-shaping the service continuum. The commonality of contemporary brief therapies relates to working with meaning making, drawing from what people bring to the process, and an important eye to how the context of people’s lives shapes distress and responses.
Let me elaborate here a bit further on brief therapy philosophy and what it suggests about how to re-shape services for children’s mental health. The brief therapy tradition misnomer has been that brevity is the goal. That is not the case although setting time limits on service has benefits for both the participant and therapist. The brevity of service in brief therapies is a consequence of our understanding of how to be with families and how to address distress. It is derivative of our working understandings about people, problems, change, and psychotherapy.
Central to brief epistemology is the practice of exercising people’s meaning making. In working with meaning making, past meanings can be re-negotiated and new meanings can be co-developed that provide a platform for the discovery of proposals for action that may not have been available pre-meeting. So there is always somewhere to go in these conversations, differences to explore and storylines to shore up. This means that each conversation in itself is therapeutic so we strive to make the most of each contact.
We embrace a general principle of utilization recognizing people bring a great deal of know-how to the process. We strive to canvas that know-how and invite people to mentor us in what they know that can be utilized and perhaps put to more agentive use. This material is described by a number of concepts including strengths, abilities, competencies, hopes, wishes, values, preferred futures, moral codes, commitments, intentions, skills for living, know-how, resources, etc. These concepts are of the local kind specific and contextual to the person’s life. These are aspects that can richly inform plans and next steps to be practiced following the therapeutic conversation.
Common among contemporary brief therapies is the location of problems as outside of people. We resist trafficking in deficit based, pathologizing bio-medical understandings of distress and embrace an understanding that problems exist outside of people in a context shaped by culture and social-relational aspects. It is an understanding and practice intimately linked to how we are always playing a role in how people come to know themselves- the identity project. This perspective moves away from practices spending time information gathering for the sake of expert driven assessment, triage, and prioritizing for wait lists. Rather each encounter is opportunity to revise identity conclusions, foreground competency, and address context.
Re-design:
Embracing these brief therapy principles a very different service pathway becomes possible. First we get face to face services up front. We meet people and begin the journey together towards preferred futures. As noted many agencies already use their walk-in counselling clinic in this capacity. In these conversations there is a ‘here and now’ and ‘where you want to go’ focus. Notes are created during the conversation and a plan or next steps are co-created. This structures the work as happening outside the session in the real world as we adopt the metaphor of practice, experimentation, trying things out, journey or project. From these conversations people may get what they need, refer to a collateral service such as Women’s Services or an Employee Assistance Program or they may schedule a follow-up to further exploration and discovery.
This process moves away from in-depth pre-service questionnaires and tools as a means to meet people to assess their lives. Instead we begin exercising meaning making skills and get on to difference and possibility. Should we encounter risk or oppression it can be addressed and safety shored up immediately inoculating against the possibility of children on wait lists living in poverty, or violence, etc.
A Proposed Service Continuum:
Putting these principles into action I propose a service continuum with two ways through the front door. The Walk-in Counselling Clinic serves as one front door to services. If people call ahead to Intake or a central point of intake service they are booked into a pre-allotted time for a Discovery Meeting.
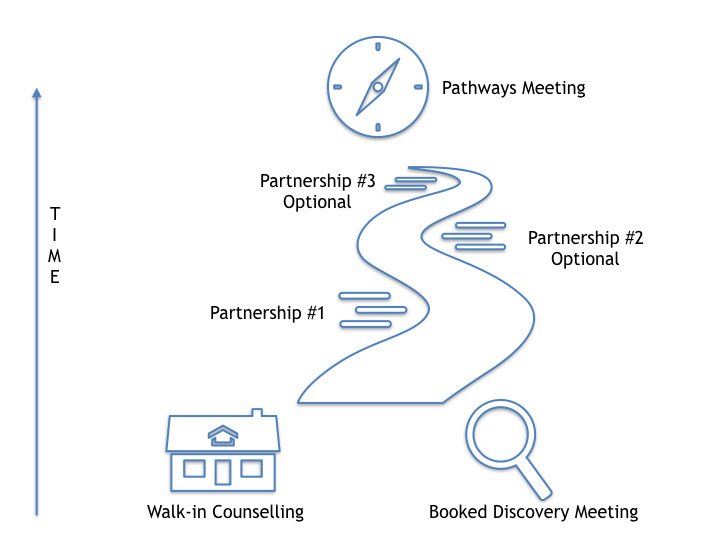
Discovery Time:
A Discovery Meeting is the first handshake with counselling services. As the title suggests it's a time to meet with a Therapist to have a conversation with purpose to discover what's possible, what might already be working, and the pathways towards a families preferred future. When families meet with the Discovery Team they begin the service journey whether that is short or long. Together they map the next steps with an eye to best fit and timing of service. This meeting is liken to a single session therapy walk-in conversation in that plans or next steps are co-developed to try out after the conversation that are derived from people’s competency and know-how.
Following the Discovery Meeting or Walk-in conversation the indv/family may get what they need and not return, could refer to a collateral agency or initiate a Partnership time. Partnership is liken to a follow-up. Entering into Partnership is a time to further the exploration of possibility together. Many people find one or two conversations is all they need to make the changes they are hoping for. In a Partnership Meeting families continue to meet with a Therapist for up to three times to further extend what is working, explore ideas to try out and different ways of thinking about things and/or themselves. These conversations assist to bring into focus the families hard work and the difference it makes. Again at any time in the Partnership stream families may end as they got what they needed, pause to continue to practice, access a collateral service that might be a better fit, or move on to a Pathways meeting to access a core service. Should a family end at this point they are always welcome to later access a Discovery Meeting to begin the process again. This ensures services are permeable and families can move in and out of services as needed.
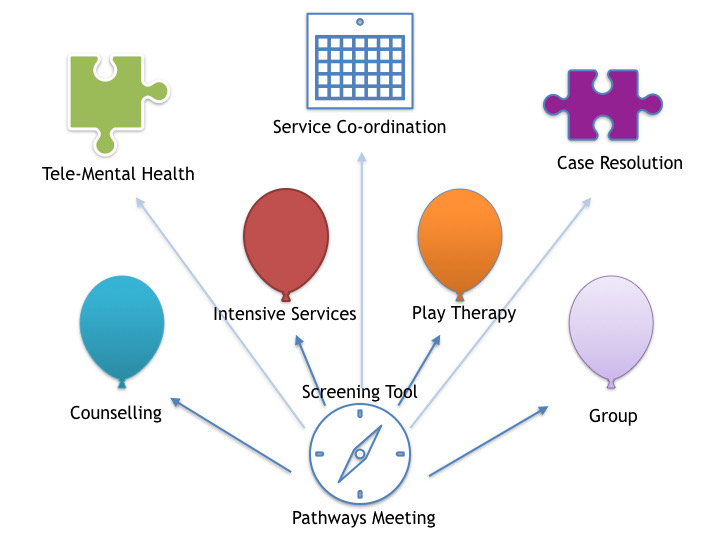
Pathways Meeting:
The Pathways Meeting involves meta-conversation. It provides a time to reflect on the journey to date and plan together to initiate further services. From the Pathways Meeting choices are collectively made in regards to ongoing services that will assist people to get towards their preferred future. The family/child/youth meets alongside their Therapist with a Pathways Therapist to plot the course ahead. This may include intensive services, ongoing counselling, time limited counselling, tele-mental health, group programs, etc. In moving on to one of these more intensive services pre and post tools may be employed to prioritize, and sift for eligibility if needed.
This service continuum strives to get useful and responsive therapeutic conversations up front along the continuum. The naming of the meetings intentionally moves away from common ways to talk about services recognizing that language is not neutral but rather shapes the picture and process for people. Discovery implies it is a time to get on to something new and different. ‘Partnership’ in contrast to ‘follow-up’ foregrounds the role each plays in the process. ‘Pathways’ implies the meeting is a time to further determine the course of service. This is in contrast to ‘intake’.
Further details in regards to how to facilitate these conversations is beyond the scope of this field note however a great deal has been written in the genre of brief narrative, solution focused brief therapy, and systemic therapy that is applicable.
